Lymphoma
Jump to navigation
Jump to search
Lymphoma is almost a specialty for itself. It can be subclassified a number of ways.
Lymphoma classification
Lymphomas can be divided into:
- Hodgkin's lymphoma.
- Non-Hodgkin's lymphoma (NHL).
Other categorizations:
- T cell lymphomas (rare).
- B cell lymphomas (more common).
Two most common NHLs:
- Follicular lymphoma (FL).
- Diffuse large B-cell lymphoma (DLBCL).
Lymphoma as a med student
- Acute lymphoid leukemia (ALL) - predominantly in smALL people, i.e. children.
- Acute myeloid leukemia (AML).
- Chronic myeloid leukemia (CML).
- Chronic lymphoid leukemia (CLL) - relatively good prognosis.
Histologic classification
- "Size".
- Nodularity.
"Size"
- The single most important factor for classifying lymphomas.
- Not really based on size.
| "Large" | "Small" | Utility | |
| Nucleoli | present | absent | most discriminative |
| Size | >2x RBC dia. | <2x RBC dia. | moderate |
| Chromatin pattern | "open" (pale) | "closed" | moderate/minimal |
| Cytoplasm | mold-minimal basophilic cytoplasm |
scant cytoplasm | minimal |
Histologic terms
- Lymphomas = cells look discohesive, may be difficult to differentiate from poor differentiated carcinoma.
- Auer rods = Acute myeloid leukemia.
- Granular cytoplasmic rod (0.5-1 x4-6 micrometres).
- Reed-Sternberg cells = Hodgkin's lymphoma.
- Large cell - very large nucleus.
- Classically binucleated.
- Large cell - very large nucleus.
- Russell bodies = Plasmacytoma (+others).
- Effacement of nodal architecture.
- Loss of proliferation centers.
IHC
General
- CD45.
- AKA common lymphocyte antigen.
- Useful to differentiate from carcinomas (e.g. small cell carcinoma).
T cell markers
- CD2 -- T cell marker (all T cells).
- CD3 -- T cell marker (all T cells).
- CD4 -- subset of T cells.
- CD8 -- subset of T cells.
- CD7 -- often lost first in T cell lymphomas.
- CD5 -- +ve in CLL & mantle cell lymphoma.
- CD43 -- +ve in mantle cell lymphoma
B cell markers
- CD20 -- B cell marker.
- CD19 -- B cell marker - used for flow cytometry.
- PAX-5.
- CD79a.
- CD10 -- follicule center.
- BCL-6.
- BCL-2.
Follicular dendritic cells
- CD23 -- follicular dendritic cells.
- CD21 -- follicular dendritic cells.
Hodgkin's lymphoma
Classic
- CD30 -- Hodgkin's lymphoma (most sensitive).
- CD15.
Hodgkin's lymphoma
Main article: Hodgkin's lymphoma
General
- Abbreviated HL.
Microscopic
By definition, HL has Reed-Sternberg cells (RSCs).
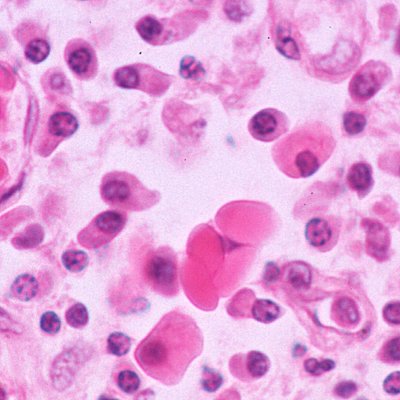
Classical HL
Features (classic HL):
- Reed-Sternberg cell.
- Large binucleated cell.
- May be multinucleated.
- May have a horseshoe-like shape.
- Macronucleolus - approximately the size of a RBC (~8 micrometers).
- Well-defined cell border.
- Large binucleated cell.
Notes:
- Large mononuclear cells are common (so called "mononuclear RSCs") but not diagnostic.
Images (classic HL):
- HL mixed cellularity - cytology (WC).
- HL mixed cellularity - cytology (WC).
- HL mixed cellularity (WC).
{kind=link}
{kind=link}
{kind=link}
Subtypes
There are four CHL subtypes:[2]
- Nodular sclerosis CHL - ~70% of CHL.
- Mixed cellular background - T cell, plasma cells, eosinophils, neutrophils and histiocytes.
- Nodular sclerosing fibrosis - thick strands fibrosis.
- Mixed cellularity CHL - ~20-25% of CHL.
- Like nodular sclerosis - but no fibrosis.
- May be associated with HIV infection.[3]
- Lymphocyte-rich CHL - rare.
- T lymphocytes only (no mix of cells).
- Lymphocyte-depleted CHL - rare.
- May be associated with HIV infection.[3]
Memory device:
- The subtypes prevalence is in reverse alphabetical order.
Nodular lymphocyte-predominant HL
Features (nodular lymphocyte-predominant Hodgkin's lymphoma):
- Popcorn cell (previously known as Lymphocytic & histiocytic cell (L&H cell)[4]) - variant of RSC:
- Cells (relatively) small (compared to classic RSCs).
- Lobulated nucleus - key feature.
- Small nucleoli.
- Subtle nodularity at low power (2.5x or 5x objective).
Images (NLPHL):
{kind=link}
Follicular lymphoma
Main article: Small cell lymphomas
Diffuse large B-cell lymphoma
Main article: Diffuse large B cell lymphoma
General
- Abbreviated DLBCL.
Microscopic
Features:[5]
- Large cells -- 4-5 times the diameter of a small lymphocytes.
- Typically have marked cell-to-cell variation in size and shape.
- Cytoplasm usu. basophilic and moderate in abundance.
- +/-Prominent nucleoli, may be peripheral and/or multiple.
Notes:
- Large bizarre cells can occasionally mimic Reed-Sternberg cells, seen in Hodgkin lymphoma.
Burkitt's lymphoma
Main article: Burkitt lymphoma
General
- Abbreviated BL.
- Subtyped by etiology.
Microscopic
Features:
- "Starry-sky pattern":
- The stars in the pattern are: tingible-body macrophages.
- Tingible-body macrophages = macrophages containing apoptotic tumour cells.
- The tumour cells are the sky.
- The stars in the pattern are: tingible-body macrophages.
- Tumour cells:[6]
- Medium-sized (~1.5-2x the size of a RBC) with uniform size ("monotonous") -- key feature.
- Round nucleus.
- Small nucleoli.
- Relatively abundant cytoplasm.
- Brisk mitotic rate.
Image: Starry-sky pattern - Ed Uthman (WC).
{kind=link}
Plasmacytoma
General
- AKA plasma cell myleoma.
- Malignancy derived from the plasma cells.
- Histologic component of multiple myeloma; to diagnose multiple myeloma other (non-pathology) criteria are needed.
- Prognosis: poor.
Microscopic
Features:
- Abundant eosinophilic cytoplasm.
- Eccentrically placed nucleus.
- Usually with "clock face" morphology.
- "Clock face" morphology = chromatin clumps around the edge of the nucleus, like the numbers on a clock face.
- May have nucleoli.
- Usually with "clock face" morphology.
- Russell bodies:
- Eosinophilic, large (10-15 micrometres), homogenous immunoglobulin-containing inclusions.
- Dutcher bodies - intranuclear crystalline rods.
- Dutcher bodies are PAS stain +ve.[7]
- Image Dutcher bodies (hematologylibrary.org).
- Prominent perinuclear hof - cytoplasmic crescent shaped lucency adjacent to the nuclear membrane (due to large Golgi apparatus); nucleus has a "bib".
{kind=link}
{kind=link}
{kind=link}
Images:
{kind=link}
DDx:
- Neuroendocrine carcinoma - nucleus often has a plasmacytoid (plasma cell-like) appearance.
Acute myeloid leukemia
General
- May afflicits young adult.
- Males>females.
Complications
- Chloroma - soft tissue mass.
- Leukostasis.
- Occurs - lungs and brain.[8]
- Hyperviscosity syndrome.
- Spontaneous bleeding with low platelet counts.
Classification
There are two classifications:
- FAB (French-American-British) - based on histologic appearance/maturation.
- WHO classification.
Histology
- Auer rods - not required to diagnose.[9]
- Cytoplasmic granular rods in blast cells.
- Dimensions: approx. 0.5-1 x 4-6 micrometres.
- Images: Auer rods (WP), Auer rods (virginia.edu).
- Cytoplasmic granular rods in blast cells.
{kind=link}
{kind=link}
Angioimmunoblastic T-cell lymphoma
Microscopic
Features:
- Clear cytoplasm.
- "Empty" sinus; subcapsular sinuses "open".
IHC
- CD7 -ve.
- CD20 +ve.
- TIA-1 -ve.
Anaplastic large cell lymphoma
General
- Abbreviated ALCL.
- May look a lot like a carcinoma.
- Often subcapsular in LNs.
- Usually T-cell derived.
- Alk IHC:
- +ve = good prognosis.
- -ve = bad prognosis.
DDx:
- Hodgkin's lymphoma.
Microscopic
Features:
- Large cells with eosinophilic cytoplasm.
- Usu. appear cohesive.
- May be subcapsular.
- Large multinucleated cell - "wreath cell" - key feature.
IHC
Features:
- Variable CD30 +ve. (???)
- CD45 +ve. (???)
Table of B-cell lymphoma
Small cell lymphomas:
| Name | Location | Size of cells | IHC | Translocations | Clinical | Other |
|---|---|---|---|---|---|---|
| Follicular lymphoma | Follicle | Small, centrocytes, centroblasts | CD10+, bcl-6+[10] | t(14,18) | Clinical ? | Other ? |
| Mantle cell lymphoma | Mantle zone | Small | CD5+, CD23-, CD43+, cyclin D1+[10] | t(11;14)(q13;q32)[11] | Clinical ? | Other ? |
| Marginal zone lymphoma (MALT) | Marginal zone | Small | CD21+, CD11c+, CD5-, CD23-[10] | Translocations | Clinical | Other |
| Precursor lymphoblastic lymphoma/leukemia | Location ? | Small | CD10+, CD5-, TdT+, CD99+[10] | Translocations ? | Clinical ? | Other ? |
Medium and large cell lymphomas:
| Name | Location | Size of cells | IHC | Translocations | Clinical | Other |
|---|---|---|---|---|---|---|
| Burkitt's lymphoma | Follicle | Large cells | CD10, bcl-6 | t(8;14) (q24;q32) | Rapid growth | "Starry sky" |
| Diffuse large B cell lymphoma | Follicle (?) | Large 4-5X of lymphocyte | MIB-1 >40% | none/like follicular l. | Poor prognosis | Common among lymphomas |
| Name | Location | Size of cells | IHC | Translocations | Clinical | Other |
See also
- Haematopathology - introduction.
References
- ↑ 1.0 1.1 Alanen A, Pira U, Lassila O, Roth J, Franklin RM (March 1985). "Mott cells are plasma cells defective in immunoglobulin secretion". Eur. J. Immunol. 15 (3): 235–42. PMID 3979421.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 567. ISBN 978-0781765275.
- ↑ 3.0 3.1 Sissolak G, Sissolak D, Jacobs P (April 2010). "Human immunodeficiency and Hodgkin lymphoma". Transfus. Apher. Sci. 42 (2): 131–9. doi:10.1016/j.transci.2010.01.008. PMID 20138008.
- ↑ Küppers R, Rajewsky K, Braeuninger A, Hansmann ML (March 1998). "L&H cells in lymphocyte-predominant Hodgkin's disease". N. Engl. J. Med. 338 (11): 763–4; author reply 764–5. doi:10.1056/NEJM199803123381113. PMID 9499174.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 676 (???). ISBN 0-7216-0187-1.
- ↑ Bellan C, Lazzi S, De Falco G, Nyongo A, Giordano A, Leoncini L (March 2003). "Burkitt's lymphoma: new insights into molecular pathogenesis". J. Clin. Pathol. 56 (3): 188–92. PMC 1769902. PMID 12610094. http://jcp.bmj.com/cgi/pmidlookup?view=long&pmid=12610094.
- ↑ URL: http://www.thefreelibrary.com/Dutcher+bodies+in+chronic+synovitis-a083551789. Accessed on: 4 August 2010.
- ↑ AML. Harrison's 16th Ed.
- ↑ AG. 8 July, 2009.
- ↑ 10.0 10.1 10.2 10.3 Lester, Susan Carole (2005). Manual of Surgical Pathology (2nd ed.). Saunders. pp. 95. ISBN 978-0443066450.
- ↑ URL: http://atlasgeneticsoncology.org/Anomalies/t1114ID2021.html. Accessed on: 10 August 2010.